José is a Data Analyst at Integrate Health. Recently, José and the Monitoring, Evaluation, and Quality Improvement team underwent a process to better understand a recent malaria supply stock-out. We asked José to tell us about that experience and how using new tools for data analysis the team was able to help Integrate Health and the government plan for the future.
Over the past year, through our data series (which you can read here), we have been sharing our experiences as we work to improve our data systems. The overarching goals of this process are to better align our data to the patient experience and measure only what is useful for program improvement. Central to these goals is using data to help us make better informed decisions and support the Government of Togo as they strengthen their health system. At Integrate Health, we believe that greater use of data to inform decision-making can help to break down silos and ensure better planning so that high-quality care can extend to even the hardest-to-reach areas—but how do we do that?
Despite major advances in national data management over the last decade, including widespread uptake of the District Health Information System (DHIS2), many low-income countries continue to struggle with ensuring enough high-quality data to forecast trends and inform healthcare delivery. As Integrate Health works in partnership with the government, filling those gaps is critical. A recent experience with supply stockouts has emphasized the importance of multiple high-quality data sources and reinforced our capacity to use data to drive decision-making.
Integrate Health collects monthly program data from Community Health Workers (CHWs) and Integrate Health-supported health centers in addition to survey data collected by our research team. In September 2020, as part of an annual health facility assessment, Integrate Health’s research team flagged that 18 out of 25 (72%) Integrate Health-supported sites reported having a stockout of malaria rapid diagnostic tests (mRDTs) in the previous four weeks. This was alarming for several reasons. First, malaria is one of the leading causes of pediatric mortality in Togo, and without mRDTs, malaria cases cannot be properly diagnosed. Second, while the stockouts were reported anecdotally to our team members as early as July, teams had little visibility into the scale of the problem. Because they were unaware of how widespread the stockouts were, they were hesitant to act. The issue was not reported in routine data collection systems. Because the stockouts were not properly recorded and thus were not reported up to the national level, opportunities to address the problem were missed.

Fortunately, by October 2020, demand for malaria testing eased as the rainy season ended, and Integrate Health-supported clinical mentors reported that facilities had sufficient mRDTs again. Nevertheless, we felt it was imperative to explore the problem to understand the root causes of the failure and identify ways to prevent it in the future. We convened a cross-functional group including members of our Programs; Operations; and Monitoring, Evaluation, and Quality Improvement teams in the US and Togo. The team identified a number of factors that contributed to the problem:
- mRDTs are purchased by the National Malaria Control Program and are delivered directly to health facilities throughout the rainy season. When one order was delayed, the results rippled throughout the country. Because mRDTs came through the National Malaria Control Program, our team had little visibility into order quantities, delivery dates, and reasons for delay. Without this information, our teams were unable to act.
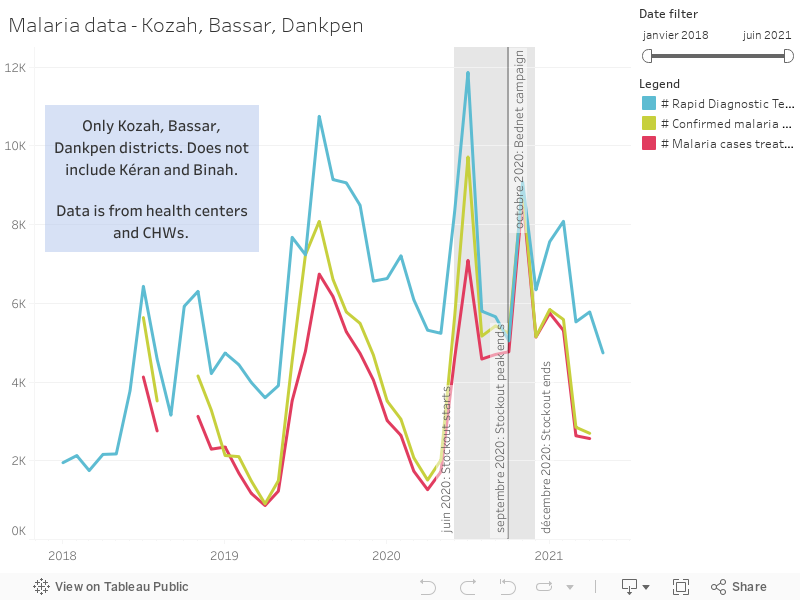
- Malaria cases spike between June and September as a result of seasonal rains. As shown in Figure 1, the number of cases of malaria diagnosed in Integrate Health-supported sites in three districts rose from 1,000 cases per month in April 2020 to over 8,000 cases per month in July 2020. The figure is a striking visualization that demonstrates the magnitude of malaria seasonality. Using data visualization tools, we were able to look at three years of malaria data, which helped us better understand the burden of malaria cases during those months.
- At the facility level, lead nurses did not report the stockouts in their routine monthly reports, which are aggregated in the national health information system, DHIS2. Nurses only reported if a stockout occurred on the day of data entry. As a result, the stock-outs did not appear in routine monitoring systems, we were not alerted early, and we failed to understand the magnitude of the problem.
As a result of these findings, we are working across teams to implement a number of actions to prevent the issue in the future and to mitigate the effect of mRDTs stockouts:
- The Monitoring, Evaluation, and Quality Improvement team reinforced training for all of the public sector nurses on how to report stockouts into the national health information system so that we can have more accurate, real-time data.
- We have shared this analysis with Integrate Health-supported CHWs, clinical staff, and Pharmacy Managers, who are now equipped to make data-informed decisions about when and where to procure extra stock of these mRDTs so that we can prevent a stockout during the next rainy season.
- We have allocated more funding to the emergency reserve of mRDTs in order to have additional supply of mRDTs on hand prior to the next rainy season. We are using the multi-year data to forecast the expected surge in cases (Figure 1).
- At the national level, our team is engaging the Ministry of Health to address the root causes of system failures that require reform at the national level, including better understanding the supply chain mechanism for the mRDTs.
Optimizing data management systems for healthcare can transform service delivery. However, many countries, including Togo, remain behind in ensuring real-time, quality data. While health information systems continue to improve, non-profit partners can play a critical role in providing additional sources of data. Integrate Health collects and analyzes data from multiple sources that can be used to better understand the full picture. Our investments in our data systems have allowed us to see multi-year trends across facilities in a way that was impossible before. This has dramatically improved our ability to forecast using real-time consumption data and to anticipate problems before they happen. As we continue to expand and improve upon our capabilities, we will continue to engage with Ministry of Health partners to use data as a tool to solve problems.
At Integrate Health, we believe that data is immensely important to decision-making. Using real-time data from the facility and national levels and effective data-capturing and visualization tools, our team has the capability to support the health system in ensuring the delivery of high-quality care. We are still improving our systems and updating our capabilities, but by being honest about the lessons we learn, we hope that others will feel bold enough to share their lessons, too. We see this as an important part of radical transparency and hope that, with it, come best practices to find solutions.